Abstract
Data on childhood cancer mortality are scarce in Burkina Faso. We estimated pediatric cancer mortality and identified its associated factors at the Yalgado Ouédraogo University Hospital Center (CHUYO) in Ouagadougou (Burkina Faso). We conducted a retrospective cohort study of children under the age of 15 admitted for cancer and treated at CHUYO between March 1, 2014, and December 31, 2017. The cumulative incidence of mortality and its associated factors were estimated with the risk of abandonment of treatment or follow-up as a competing risk. A total of 168 children/adolescents were included at a median age of 7 years (interquartile range [IQR]: 4–10 years); 71% were boys. The median follow-up duration was 4.51 person-months (IQR: 1.85-10.5). Burkitt lymphoma (77%) and retinoblastoma (21%) were the most common cancer. The majority of Burkitt lymphoma (90%) were diagnosed at stage 3/4; the abdominal (58%) and maxillofacial (23%) locations were the most common. All children/adolescents received chemotherapy and 10% received chemotherapy and surgery. No patients received radiotherapy. During follow-up, overall mortality was 46%, and the risk of abandonment was 39%. The cumulative incidence of mortality was 30, 43, and 45 per 100 person-months at 6, 12, and 24 months, respectively. In multivariate analysis, male gender (adjusted sub hazard ratio [aSHR]: 2.20; 95%CI: 1.13-4.27), abdominal localization (aSHR: 2.68; 95%CI: 1.24-5.78), maxillofacial and abdominal localization (aSHR: 3.39; 95%CI: 1.42-8.09) increased significantly the risk of death among children and adolescent treated for Burkitt lymphoma. Early diagnosis and improved access to treatment are essential for better survival rates among children and adolescents with cancer in Burkina Faso.
|
Published in
|
Central African Journal of Public Health (Volume 11, Issue 6)
|
|
DOI
|
10.11648/j.cajph.20251106.12
|
|
Page(s)
|
343-351 |
|
Creative Commons
|

This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
|
|
Copyright
|
Copyright © The Author(s), 2025. Published by Science Publishing Group
|
Keywords
Childhood Cancers, Mortality, Associated Factors, Burkina Faso
1. Introduction
According to the Lancet Oncology Commission, there will be 13.7 million new cases of childhood cancer globally between 2020 and 2050. Among them, 6.1 million (44.9%) of these children will be undiagnosed and 11.1 million children will die from cancer if no additional investments are made to improve access to health-care services or childhood cancer treatment. Of this total, 9.3 million children (84.1%) will be in low-income and lower-middle-income countries
| [1] | Ward ZJ, Yeh JM, Bhakta N, et al. Estimating the total incidence of global childhood cancer: a simulation-based analysis. Lancet Oncol 2019; 20: 483–493. |
| [2] | Atun R, Bhakta N, Denburg A, et al. Sustainable care for children with cancer: a Lancet Oncology Commission. Lancet Oncol 2020; 21: e185–e224. |
[1, 2]
. Thus, the childhood cancer burden is disproportionally concentrated in low- and middle-income countries (LMICs). In these settings, inadequate health-care infrastructure and service delivery capabilities, limited access to quality medicines, an inadequate multidisciplinary health workforce, low quality of care, adverse socioeconomic environments, cultural and educational barriers, and a low level of awareness result in missed diagnosis, delayed diagnosis, underdiagnosis, and suboptimal care of childhood cancer
| [2] | Atun R, Bhakta N, Denburg A, et al. Sustainable care for children with cancer: a Lancet Oncology Commission. Lancet Oncol 2020; 21: e185–e224. |
| [5] | De Angelis C, Pacheco C, Lucchini G, et al. The experience in nicaragua: childhood leukemia in low income countries-the main cause of late diagnosis may be ‘medical delay’. Int J Pediatr 2012; 2012: 129707. |
[2–5]
. Consequently, in LMICs, childhood cancer survival rates are thought not to exceed 30%, compared to around 80% in high-income countries
| [6] | Ward ZJ, Yeh JM, Bhakta N, et al. Global childhood cancer survival estimates and priority-setting: a simulation-based analysis. Lancet Oncol 2019; 20: 972–983. |
| [7] | Gatta G, Botta L, Rossi S, et al. Childhood cancer survival in Europe 1999-2007: results of EUROCARE-5--a population-based study. Lancet Oncol 2014; 15: 35–47. |
[6, 7]
. In light of these disparities and high mortality in LMICS, specially in Sub-Saharan Africa, in 2018 the World Health Organization (WHO) launched the Global Initiative for Childhood Cancer (GICC), with the goal of attaining at least 60% cancer survival for children worldwide by the year 2030
.
In Africa, and particularly in Burkina Faso, childhood cancers, once considered rare, are now emerging due to improvement in diagnostic capabilities, contributing to an increase in children mortality
| [9] | Ngwa W, Addai BW, Adewole I, et al. Cancer in sub-Saharan Africa: a Lancet Oncology Commission. Lancet Oncol 2022; 23: e251–e312. |
[9]
. Nephroblastoma, retinoblastoma, and Burkitt's lymphoma are the most common cancers in Africa
. Despite being highly curable, the estimates of 5-year net survival among diagnosed childhood cancer cases in Africa were only 19% in southern Africa and 8% in both eastern and western Africa
| [6] | Ward ZJ, Yeh JM, Bhakta N, et al. Global childhood cancer survival estimates and priority-setting: a simulation-based analysis. Lancet Oncol 2019; 20: 972–983. |
[6]
. To address this high mortality rate, diverse initiatives emerged in recent decades in Africa. In 2005, Burkina Faso joined the Franco-African Pediatric Oncology Group (GFAOP) created in 2002 to support African countries in the treatment of childhood cancer
. Membership of the GFAOP has led to improvements in the treatment of childhood cancers in Burkina Faso
. However, childhood cancer data remains scare.
Since the launch of the GICC, few countries have reported baseline data of survival for the childhood cancer. In Africa, the survival rates were between 26.9% to 77.9% for nephroblastoma, between 23% to 100% for retinoblastoma, 45% to 95% for Hodgkin lymphoma and 28% to 76% for Burkitt lymphoma
| [12] | van Heerden J, Balagadde-Kambugu J, Angom R, et al. Evaluating the baseline survival outcomes of the “six Global Initiative for Childhood Cancer index cancers” in Africa. Pediatr Hematol Oncol 2023; 40: 203–223. |
[12]
. In Malawi, among 264 children with cancer treated, 52% were alive without evidence of disease
| [13] | Chakumatha E, Weijers J, Banda K, et al. Outcome at the end of treatment of patients with common and curable childhood cancer types in Blantyre, Malawi. Pediatr Blood Cancer 2020; 67: e28322. |
[13]
. There has been little research in childhood cancer treatment outcomes in Burkina Faso. The objective of this study was to estimate the mortality and to identify factors associated with mortality in children and adolescents diagnosed and treated for pediatric cancer in Ouagadougou (Burkina Faso).
2. Methods
2.1. Study Design, Setting and Participant
We conducted a retrospective cohort study of children/adolescents under the age of 15 diagnosed and treated for childhood cancer between January 1, 2014, and December 31, 2017, at the Yalgado Ouédraogo University Hospital Center in Ouagadougou (Burkina Faso).
CHUYO is one of four referral hospitals in Burkina Faso. It comprises 10 departments, including Pediatrics. The Pediatrics Department had five units including the pediatric oncology unit. The pediatric oncology unit had six inpatient rooms with a capacity of 28 beds. Patient care was provided by two pediatricians, assisted by doctors specializing in pediatrics, nurses, and medical interns.
As part of the GFAOP initiative, which targets the five main curable childhood cancers in Africa, three cancers are treated at CHUYO (Burkitt lymphoma, Hodgkin lymphoma, and retinoblastoma) and two at CHU Charles De Gaulle (Acute Lymphoblastic Leukemia and nephroblastoma). In addition to these cancers, these centers also treat other types of childhood cancer. Cancer drugs are provided by the GFAOP. For drugs that are unavailable, parents must contribute financially to the care of their children. Treatment is organized in the form of cures. Between cures, patients are often allowed to leave temporarily and return for their next cure. At the end of treatment, regular scheduled appointments allow for monitoring of the cancer's progression.
All children aged 0 to 15 years who were admitted and treated in the pediatric oncology unit of the CHUYO for cancer between January 1, 2014, and December 31, 2017 were eligible for this study. Children whose clinical records were insufficiently detailed and therefore unusable were not included.
2.2. Study Variables
Study variables were extracted in children/adolescent record. We extracted sociodemographic data (child/adolescent age, gender, country of residence, place of residence, caregiver’s occupation), type of cancer, stage of the cancer, cancer localization, cancer treatment data (date of the cancer diagnosis, date of the cancer treatment), type of treatment (chemotherapy, radiotherapy, surgery), and treatment outcomes (alive, deceased, and abandonment).
2.3. Statistical Analysis
Categorical variables were described using frequencies and percentages, and comparisons between groups were performed using the chi-square test or Fisher’s exact test, as appropriate. Continuous variables were summarized using medians and interquartile ranges (IQR), and group comparisons were performed using the Wilcoxon rank-sum test.
The incidence of death was estimated for 100 person-months with it 95% confidence interval (95%CI). Follow-up time was calculated from the date of treatment to the date of last medical visit for those alive, death or abandonment. The date of entry into the cohort was the date of diagnosis confirmed by the medical report. Outcome at end of follow-up was categorized as: alive (complete or partial remission of cancer), treatment abandonment, and death reported in medical record or reported by parents. The abandonment was defined as discharged against medical advice, or patients discharged with medical advice and not seen at follow-up by December 31, 2018. The end date of follow-up was December 31, 2018.
In this analysis, the outcome of interest was death, which was analyzed in competition with “abandonment”. Patients who were alive at the end of treatment, or abandoned the treatment were censored at the date of discharge or last contact. To identify predictors of mortality for children and adolescents treated for Burkitt Lymphoma, we used a competing risk survival model based on the Fine and Gray subdistribution hazard method
| [15] | Stefan C, Bray F, Ferlay J, et al. Cancer of childhood in sub-Saharan Africa. ecancermedicalscience 2017; 11: 755. |
[15]
. In univariable analysis, variables associated with death at the 20% threshold were retained for multivariable analysis. A backward stepwise selection strategy was applied to identify independent predictors of mortality at the 5% significance level in the multivariable analysis. All analyses were performed using SAS 9.4 (SAS Institute Inc., Cary, NC, USA).
2.4. Ethical Considerations
This study used data collected for clinical purposes and public health surveillance. Because of a legitimate public health purpose, the ethical approval and the informed consent was not required for this study. To assure the anonymity, we did not collect patient’s name; we used a unique identifier.
3. Results
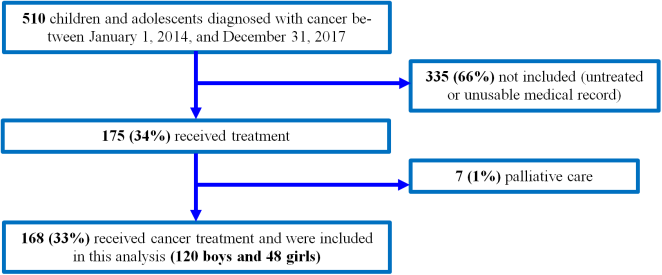
Between January 1, 2014, and December 31, 2017, 510 children and adolescents were diagnosed with cancer and admitted in CHUYO pediatric oncology unit. Of these, 335 (66%) untreated or with unusable medical record and 7 (1%) whom received only palliative treatment were not included in this analysis. Overall, 168 (34%) received cancer treatment and were enrolled in the study. The majority of children/adolescents were male (71%, 120/168). (
Figure 1)
Figure 1. Flow chart of the inclusion process of children and adolescent with cancer eligible for this study (Ouagadougou, January 1, 2014, and December 31, 2017).
3.1. Sociodemographic and Clinical Characteristics
The median age of participants was 7 years (IQR: 4–10 years). The majority of the participants came from rural area (81%). Theirs parents were mostly farmers/breeder for the fathers and housewives for the mothers. These sociodemographic characteristics did not differ significantly between the genders. (
Table 1)
The most common childhood cancers were Burkitt lymphoma (77%) and retinoblastoma (21%). Most of the Burkitt Lymphoma were diagnosed at stage 3 (57%) or stage 4 (41%). The proportion stage 3 or 4 Burkitt Lymphoma cancer were significantly greater for male compared to female (p=0.04). The two cases of neuroblastoma and the case of Hodgkin lymphoma were at stage 2. The Burkitt lymphoma were localized mostly in the abdomen (58%). All children and adolescents were treated by chemotherapy. In addition, 10% were treated by surgery. No children/adolescents were treated with radiotherapy. These later characteristics did not differ significantly between the gender. (
Table 1)
Table 1. Sociodemographic and clinical characteristics of children and adolescents treated for childhood cancer at the Yalgado Ouédraogo University Hospital Center in Ouagadougou, from January 1, 2014, and December 31, 2017, according to gender.
| Gender | TOTAL |
Female Frequency (%) | Male Frequency (%) | p | Frequency (%) |
Age in years | | | 0,92 | |
[0-5[ | 15 (31,3) | 35 (29,2) | | 50 (29,8) |
[5-10[ | 20 (41,7) | 49 (40,8) | | 69 (41,1) |
[10-15] | 13 (27,1) | 36 (30,0) | | 49 (29,2) |
Father's occupation | | | 0,26 | |
Farmer/Breeder | 36 (75,0) | 99 (82,5) | | 135 (80,4) |
Other | 12 (25,0) | 21 (17,5) | | 33 (19,6) |
Mother's occupation | | | 0,32 | |
Housewife | 46 (95,8) | 118 (98,3) | | 164 (97,6) |
Other | 2 (4,2) | 2 (1,7) | | 4 (2,4) |
Country of residence | | | 1 | |
Burkina Faso | 43 (89,6) | 108 (90,0) | | 151 (89,9) |
Côte d’Ivoire | 5 (10,4) | 12 (10,0) | | 17 (10,1) |
Aera of residence | | | 0,09 | |
Rural | 35 (72,9) | 101 (84,2) | | 136 (81,0) |
Urbain | 13 (27,1) | 19 (15,8) | | 32 (19,0) |
Type of cancer | | | 0,15 | |
Burkitt lymphoma | 37 (77,1) | 93 (77,5) | | 130 (77,4) |
Hodgkin lymphoma | - | 1 (0,8) | | 1 (0,6) |
Neuroblastoma | 2 (4,2) | - | | 2 (1,2) |
Retinoblastoma | 9 (18,8) | 26 (21,7) | | 35 (20,8) |
Stage of Burkitt lymphoma | | | 0.04 | |
Stage 2 | 2 (15.4) | 11 (84.6) | | 13 (10.0) |
Stage 3 | 28 (36.8) | 48 (63.2) | | 76 (56.5) |
Stage 4 | 7 (17.1) | 34 (82.9) | | 41 (41.5) |
Localization of Burkitt lymphoma | | | 0.11 | |
Abdominal | 25 (32.9) | 51 (67.1) | | 76 (58.5) |
Maxillo-facial | 4 (13.3) | 26 (86.7) | | 30 (23.1) |
Maxillo-facial and abdominal | 8 (33.3) | 16 (66.7) | | 24 (18.4) |
Chemotherapy | 48 (100) | 120 (100) | | 168 (100) |
Surgery | 5 (10,4) | 12 (10,0) | | 17 (10,1) |
3.2. Mortality Rate and Its Associated Factors
Over the study period, 77 (45.8%) deceased, 66 (39.3%) abandoned and 25 (14.9%) were alive (22 in complete and 3 in partial remission). The cumulative incidence of mortality did not differ according to cancer type. (
Table 2)
Table 2. Treatment outcomes among children and adolescents treated for childhood cancer at the Yalgado Ouédraogo University Hospital Center in Ouagadougou, from January 1, 2014, and December 31, 2017, according to cancer type.
| Alive Frequency (%) | Deceased Frequency (%) | Abandonment Frequency (%) | p-value | Total |
Type of cancer | | | | 0.64 | |
Burkitt lymphoma | 18 (13.9) | 61 (46.9) | 51 (39.2) | | 130 |
Hodgkin lymphoma | 0 (0.0) | 0 (0.0) | 1 (100.0) | | 1 |
Neuroblastoma | 0 (0.0) | 2 (100.0) | 0 (0.0) | | 2 |
Retinoblastoma | 7 (20.0) | 14 (40.0) | 14 (40.0) | | 35 |
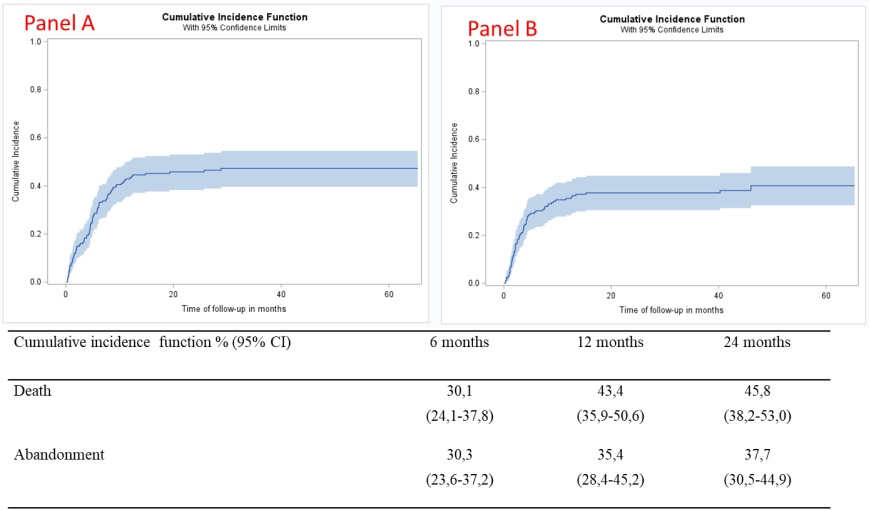
The total follow-up time for the 168 participants was 1745 person-months. The median follow-up time was 4.51 person-months (IQR: 1.85-10.5). The overall mortality rate was 47 per 100 person-months (95%CI: 39 to 54 person-months). While the overall abandonment rate was 41 per 100 person-months (95% CI: 32 to 49 person-months). (
Figure 2)
The mortality rate for Burkitt Lymphoma was 31 per 100 person-months (95%CI: 23-38 person-months), 43 person-months (95%CI: 34-51 person-months), 45 person-months (95%CI: 36-54 person-months), 47 person-months (95%CI: 38-55 person-months person-months) at 6, 12, 24 and 60 months, respectively. The mortality rate for retinoblastoma was 25 per 100 person-months (95%CI: 12-41 person-months), 37 person-months (95%CI: 21-53 person-months), 41 person-months (95%CI: 24-57 person-months), at 6, 12, 24 and 36 months, respectively.
Figure 2. Cumulative incidence of death (panel A) and abandonment (panel B) of children and adolescents treated for childhood cancer at the Yalgado Ouédraogo University Hospital Center in Ouagadougou, from January 1, 2014, and December 31, 2017.
In the multivariable competing risks model, gender and cancer localization were independently associated with the risk of death among children and adolescent treated for Burkitt lymphoma. Compared with female, male had a significantly higher risk of mortality (adjusted sub hazard ratio [aSHR]: 2.20; 95% CI: 1.13-4.27). Compared with those with maxillo-facial cancer, the abdominal (aSHR: 2.68 ; 95%CI: 1.24-5.78) and maxillo-facial localization (aSHR: 3.39; 95%CI: 1.42-8.09) were associated with increased mortality risk. (
Table 3)
Table 3. Factors associated with mortality among children and adolescents treated for Burkitt Lymphoma at the Yalgado Ouédraogo University Hospital Center in Ouagadougou, from January 1, 2014, and December 31, 2017. (Univariable and multivariable competing risk regression analysis).
| SHR | IC95% | p-value | aSHR | IC95% | p-value |
Age in years | | | 0.28 | | | |
[0-5[ | | | | | | |
[5-10[ | 1.30 | 0.65-2.62 | | | | |
[10-15] | 0.84 | 0.41-1.71 | | | | |
Sexe | | | 0.06 | | | 0,02 |
Female | | | | 1 | | |
Male | 1.83 | 0.96-3.45 | | 2.20 | 1.13-4.27 | |
Father's occupation | | | 0.94 | | | |
Farmer/Breeder | 1.02 | 0.50-2.10 | | | | |
Other | | | | | | |
Country of residence | | | 0.98 | | | |
Burkina Faso | | | | | | |
Côte d’Ivoire | 0.99 | 0.42-2.31 | | | | |
Place of residence | | | 0.82 | | | |
Rural | 1 | | | | | |
Urban | 1.09 | 0.52-2.26 | | | | |
Localization du cancer | | | 0.04 | | | 0.02 |
Maxillo-facial | 1 | | | 1 | | |
Abdominal | 2.32 | 1.09-4.94 | | 2.68 | 1.24-5.78 | |
Maxillo-facial et abdominal | 2.79 | 1.18-6.62 | | 3.39 | 1.42-8.09 | |
Stage of Burkitt lymphoma | | | | | | |
Stage 2 | 1 | | 0.55 | | | |
Stage 3 | 1.60 | 0.53-4.78 | | | | |
Stage 4 | 1.82 | 0.60-5.56 | | | | |
SHR: sub hazard ratio; aSHR: adjusted sub hazard ratio; 95%CI: 95% interval confidence
4. Discussion
Our study aim was to estimate the survival and to identify factors associated with mortality in children and adolescents diagnosed and treated for childhood cancer in Ouagadougou (Burkina Faso). The main cancers diagnosed and treated was Burkitt lymphoma (74%) and retinoblastoma (21%). Our results highlight a high rate of mortality estimated at 47 per 100 person-months. In addition, we report a high rate of treatment and follow-up abandonment estimated at 41 per 100 person-months. This high mortality was associated with gender and cancer localization for Burkitt lymphoma.
Burkitt lymphoma and retinoblastoma were the most frequent cancer among our study participants. Burkitt lymphoma is an aggressive, fast-growing cancer of the lymphatic system. It is highly associated with the Epstein-Barr virus (EBV) and endemic malaria, which explains its high prevalence in our setting
| [14] | Hämmerl L, Colombet M, Rochford R, et al. The burden of Burkitt lymphoma in Africa. Infect Agent Cancer 2019; 14: 17. |
| [15] | Stefan C, Bray F, Ferlay J, et al. Cancer of childhood in sub-Saharan Africa. ecancermedicalscience 2017; 11: 755. |
[14, 15]
. Retinoblastoma, the most common primary intraocular malignancy in children, burden is also disproportionately high in Africa. In fact, several African studies report a higher incidence of these two cancers in the pediatric oncologic units
| [16] | Lukamba RM, Yao J-JA, Kabesha TA, et al. Retinoblastoma in Sub-Saharan Africa: Case Studies of the Republic of Côte d’Ivoire and the Democratic Republic of the Congo. J Glob Oncol 2018; 4: JGO.17.00056. |
| [17] | Sherief ST, Asfaw G, Abateneh A, et al. Incidence and geographic distribution of retinoblastoma in Ethiopia. BMC Ophthalmol 2023; 23: 231. |
[16, 17]
. However, it is important to note that the actual incidence of these cancers is underestimated in our context. In our study many patients diagnosed had not been treated and several medical records were incomplete. Several barriers hinder the accurate estimation of the childhood cancer in our context. Burkina Faso lacks mandatory nationwide cancer registration systems. In addition, for poor populations disproportionally affected by these cancers as reported by our data, healthcare could be inaccessible because of poverty, long distances to specialized centers, and high treatment costs
| [18] | Ritter J, Allen S, Cohen PD, et al. Financial hardship in families of children or adolescents with cancer: a systematic literature review. Lancet Oncol 2023; 24: e364–e375. |
[18]
. Others barriers are cultural beliefs and stigma surrounding cancers. These later can lead families to seek traditional healers first, thus delaying modern medical diagnosis until the disease is very advanced
| [19] | Stoeter O, Mezger NCS, Koenig T, et al. Self-Perceived Barriers to Pediatric Cancer Care in Sub-Saharan Africa: A Cross-Sectional Multinational Study. JCO Glob Oncol 2025; e2400137. |
| [20] | Abdelkhalek E, Sherief L, Kamal N, et al. Factors associated with delayed cancer diagnosis in egyptian children. Clin Med Insights Pediatr 2014; 8: 39–44. |
[19, 20]
. It is essential to invest in the development of cancer registries in Burkina Faso that incorporate childhood cancers. These data and evidence are important for guiding country priorities and actions to address childhood cancers
| [2] | Atun R, Bhakta N, Denburg A, et al. Sustainable care for children with cancer: a Lancet Oncology Commission. Lancet Oncol 2020; 21: e185–e224. |
[2]
.
In our study, a high proportion of children/adolescent with cancer have advanced disease at presentation. They were most often at stage 3 and 4. The proportion of stage 3 or 4 was greater for males compared to female. This late presentation already reported in previous study
| [20] | Abdelkhalek E, Sherief L, Kamal N, et al. Factors associated with delayed cancer diagnosis in egyptian children. Clin Med Insights Pediatr 2014; 8: 39–44. |
| [21] | Brown BJ, Ajayi SO, Ogun OA, et al. Factors influencing time to diagnosis of childhood cancer in Ibadan, Nigeria. Afr Health Sci 2009; 9: 247–253. |
[20, 21]
, is related to barriers to healthcare presented above. Most childhood cancers are very aggressive and develop rapidly. This late presentation could also be explained by the therapeutic errancy related to inadequate awareness of cancer by front-line health-care workers, understaffing of primary health facilities, and lack of referral mechanisms
| [21] | Brown BJ, Ajayi SO, Ogun OA, et al. Factors influencing time to diagnosis of childhood cancer in Ibadan, Nigeria. Afr Health Sci 2009; 9: 247–253. |
| [22] | Brasme J-F, Morfouace M, Grill J, et al. Delays in diagnosis of paediatric cancers: a systematic review and comparison with expert testimony in lawsuits. Lancet Oncol 2012; 13: e445-459. |
[21, 22]
. The consequence of this late presentation is a high mortality reported in our study, which included cancers that are curable if treated early. In fact, in this cohort, after a median follow-up time of 4.51 person-months, the mortality rate was 47 per 100 person-months. While the overall abandonment rate was 41 per 100 person-months. This low rate of survival was previously reported in West Africa
| [23] | Utuk E-OE, Ikpeme EE. Childhood cancers in a referral hospital in south-south nigeria: a review of the spectrum and outcome of treatment. Pan Afr Med J; 22. Epub ahead of print 2 December 2015. https://doi.org/10.11604/pamj.2015.22.325.6990 |
[23]
. Specifically, the mortality rate for Burkitt Lymphoma was 47 person-months at 60 months. That of retinoblastoma was 41 person-months at 36 months. These survival rates remain significantly lower than the GICC goal of at least 60% cancer survival the overall survival. It is also lower than the rate of 42 to 60% reported by the GFAOP, in South Africa, Uganda, and in Malawi
| [13] | Chakumatha E, Weijers J, Banda K, et al. Outcome at the end of treatment of patients with common and curable childhood cancer types in Blantyre, Malawi. Pediatr Blood Cancer 2020; 67: e28322. |
| [24] | Ozuah NW, Lubega J, Allen CE, et al. Five decades of low intensity and low survival: adapting intensified regimens to cure pediatric Burkitt lymphoma in Africa. Blood Adv 2020; 4: 4007–4019. |
| [26] | Liu B, Youlden DR, Wabinga H, et al. Survival from childhood cancer in Kampala, Uganda. Pediatr Blood Cancer 2021; 68: e28876. |
[13, 24–26]
. To reduce this high mortality, it is urgent to promote equity of access in healthcare in sub-Saharan Africa, particularly in Burkina Faso. A universal health coverage, incorporating cancer care into essential benefits packages and national health insurance systems to reduce out-of-pocket expenditures for essential therapies for citizens with cancer is a possible action to reduce this mortality
| [9] | Ngwa W, Addai BW, Adewole I, et al. Cancer in sub-Saharan Africa: a Lancet Oncology Commission. Lancet Oncol 2022; 23: e251–e312. |
[9]
.
Our study highlights a treatment abandonment as a big issue for childhood cancer treatment in Burkina Faso. Abandonment of treatment is a socioeconomic issue as a medical one, and is often the result of various factors beyond the control of the patients and parents
| [27] | Mostert S, Arora RS, Arreola M, et al. Abandonment of treatment for childhood cancer: position statement of a SIOP PODC Working Group. Lancet Oncol 2011; 12: 719–720. |
[27]
. Treatment abandonment contributes to the low survival rates. This high abandonment rates have been documented in previous study in Sub-Saharan Africa
| [28] | Mansell R, Purssell E. Treatment abandonment in children with cancer in Sub-Saharan Africa: Systematic literature review and meta-analysis. J Adv Nurs 2018; 74: 800–808. |
[28]
. Cancer treatment abandonment underlying reasons include intolerable stigma, inability to pay for treatment, and high transport and accommodation costs
| [28] | Mansell R, Purssell E. Treatment abandonment in children with cancer in Sub-Saharan Africa: Systematic literature review and meta-analysis. J Adv Nurs 2018; 74: 800–808. |
[28]
. The scale up of interventions addressing the financial, logistical, educational, and systemic barriers faced by families and health care workers could be an effective strategy to mitigate cancer treatment in Africa.
Our results show that boys were at higher risk of mortality compared with girls. This trend is observed in both incidence and mortality rates, with boys experiencing more cancer diagnoses at advanced stage and deaths in our study. This result is consistent with data from the literature showing that childhood cancer mortality is generally higher for boys than for girls
| [29] | Williams LA, Spector LG. Survival Differences Between Males and Females Diagnosed With Childhood Cancer. JNCI Cancer Spectr 2019; 3: pkz032. |
[29]
. These results could be explained by biological and genetical factors. Further research is needed to study the genetic susceptibility in childhood cancer in sub-Saharan Africa. We also show that compared to maxilla-facial localization, abdominal localization and maxillo-abdominal increased the risk of death among those with Burkitt lymphoma. The Burkitt lymphoma presentations in abdomen are frequently associated with high tumor burden and advanced disease. They can cause severe complications such as bowel obstruction, intussusception, perforation, or massive ascites, which constitute oncologic emergencies. In addition, a large abdominal mass is a poor prognostic sign due to the high risk of tumor lysis syndrome during chemotherapy and the technical difficulty of completely resecting the tumor
| [30] | Molyneux EM, Rochford R, Griffin B, et al. Burkitt’s lymphoma. The Lancet 2012; 379: 1234–1244. |
[30]
.
Our study has some limitations. Several patients were not included because they medical records were incomplete or they did not receive cancer treatment. This could lead to selection bias resulting in an underestimation of cancer cases and mortality rates. In addition, we conduct this study only in CHUYO in Ouagadougou. Our participants are not representative of children and adolescents with cancer in Burkina Faso. Despite these limitations, our study which used a robust design and analyzed the data by treating abandonment as an adverse event and by censoring cases at the time of abandonment is original and fills a gap in data on pediatric cancers in Burkina Faso.
5. Conclusion
Our study reported a high rate of treatment and follow-up abandonment and a high rate of mortality among children and adolescent treated for cancer in the CHUYO in Ouagadougou (Burkina Faso). Interventions to enable parents to complete treatment and follow-up of their child and improved supportive care are needed. Improvements in screening and treatment are also needed. All of this will contribute to a significant reduction in cancer-related infant mortality.
Abbreviations
95%CI | 95% Confidence Interval |
aSHR | Adjusted Sub Hazard Ratio |
GFAOP | Franco-African Pediatric Oncology Group |
GICC | Global Initiative for Childhood Cancer |
IQR | Interquartile Range |
LMICs | Low- and Middle-Income Countries |
WHO | World Health Organization |
Acknowledgments
We would like to thank the staff of CHUYO Oncology unit, children, adolescents and their parents.
Author Contributions
Dahourou Désiré Lucien: Conceptualization, Formal Analysis, Methodology, Software, Supervision, Writing – original draft, Writing – review & editing
Kalmogho Angèle: Conceptualization, Methodology, Supervision, Validation, Writing – review & editing
Kabore Rolande: Validation, Writing – review & editing
Yonaba Caroline: Conceptualization, Methodology, Supervision, Validation, Writing – review & editing
Bouda Chantal: Validation, Writing – review & editing
Bouda Charlotte: Data curation, Validation, Writing – review & editing
Zoungrana Chantal: Validation, Writing – review & editing
Ouédraogo Flore: Validation, Writing – review & editing
Kouéta Fla: Supervision, Validation, Writing – review & editing
Conflicts of Interest
The authors declare that there is no conflict of interest.
References
| [1] |
Ward ZJ, Yeh JM, Bhakta N, et al. Estimating the total incidence of global childhood cancer: a simulation-based analysis. Lancet Oncol 2019; 20: 483–493.
|
| [2] |
Atun R, Bhakta N, Denburg A, et al. Sustainable care for children with cancer: a Lancet Oncology Commission. Lancet Oncol 2020; 21: e185–e224.
|
| [3] |
Leal-Leal CA, Dilliz-Nava H, Flores-Rojo M, et al. First contact physicians and retinoblastoma in Mexico. Pediatr Blood Cancer 2011; 57: 1109–1112.
|
| [4] |
Rodriguez-Galindo C, Friedrich P, Morrissey L, et al. Global challenges in pediatric oncology. Curr Opin Pediatr 2013; 25: 3–15.
|
| [5] |
De Angelis C, Pacheco C, Lucchini G, et al. The experience in nicaragua: childhood leukemia in low income countries-the main cause of late diagnosis may be ‘medical delay’. Int J Pediatr 2012; 2012: 129707.
|
| [6] |
Ward ZJ, Yeh JM, Bhakta N, et al. Global childhood cancer survival estimates and priority-setting: a simulation-based analysis. Lancet Oncol 2019; 20: 972–983.
|
| [7] |
Gatta G, Botta L, Rossi S, et al. Childhood cancer survival in Europe 1999-2007: results of EUROCARE-5--a population-based study. Lancet Oncol 2014; 15: 35–47.
|
| [8] |
Global initiative for childhood cancer,
https://www.who.int/publications/m/item/global-initiative-for-childhood-cancer
(accessed 19 August 2025).
|
| [9] |
Ngwa W, Addai BW, Adewole I, et al. Cancer in sub-Saharan Africa: a Lancet Oncology Commission. Lancet Oncol 2022; 23: e251–e312.
|
| [10] |
Accueil. GFAOP,
https://www.gfaop.org/
(accessed 19 August 2025).
|
| [11] |
Cancer Control FRANCOPHONE 2021 - Cancer Control,
https://www.cancercontrol.info/cancer-control-francophone-2021-2/
(2021, accessed 19 August 2025).
|
| [12] |
van Heerden J, Balagadde-Kambugu J, Angom R, et al. Evaluating the baseline survival outcomes of the “six Global Initiative for Childhood Cancer index cancers” in Africa. Pediatr Hematol Oncol 2023; 40: 203–223.
|
| [13] |
Chakumatha E, Weijers J, Banda K, et al. Outcome at the end of treatment of patients with common and curable childhood cancer types in Blantyre, Malawi. Pediatr Blood Cancer 2020; 67: e28322.
|
| [14] |
Hämmerl L, Colombet M, Rochford R, et al. The burden of Burkitt lymphoma in Africa. Infect Agent Cancer 2019; 14: 17.
|
| [15] |
Stefan C, Bray F, Ferlay J, et al. Cancer of childhood in sub-Saharan Africa. ecancermedicalscience 2017; 11: 755.
|
| [16] |
Lukamba RM, Yao J-JA, Kabesha TA, et al. Retinoblastoma in Sub-Saharan Africa: Case Studies of the Republic of Côte d’Ivoire and the Democratic Republic of the Congo. J Glob Oncol 2018; 4: JGO.17.00056.
|
| [17] |
Sherief ST, Asfaw G, Abateneh A, et al. Incidence and geographic distribution of retinoblastoma in Ethiopia. BMC Ophthalmol 2023; 23: 231.
|
| [18] |
Ritter J, Allen S, Cohen PD, et al. Financial hardship in families of children or adolescents with cancer: a systematic literature review. Lancet Oncol 2023; 24: e364–e375.
|
| [19] |
Stoeter O, Mezger NCS, Koenig T, et al. Self-Perceived Barriers to Pediatric Cancer Care in Sub-Saharan Africa: A Cross-Sectional Multinational Study. JCO Glob Oncol 2025; e2400137.
|
| [20] |
Abdelkhalek E, Sherief L, Kamal N, et al. Factors associated with delayed cancer diagnosis in egyptian children. Clin Med Insights Pediatr 2014; 8: 39–44.
|
| [21] |
Brown BJ, Ajayi SO, Ogun OA, et al. Factors influencing time to diagnosis of childhood cancer in Ibadan, Nigeria. Afr Health Sci 2009; 9: 247–253.
|
| [22] |
Brasme J-F, Morfouace M, Grill J, et al. Delays in diagnosis of paediatric cancers: a systematic review and comparison with expert testimony in lawsuits. Lancet Oncol 2012; 13: e445-459.
|
| [23] |
Utuk E-OE, Ikpeme EE. Childhood cancers in a referral hospital in south-south nigeria: a review of the spectrum and outcome of treatment. Pan Afr Med J; 22. Epub ahead of print 2 December 2015.
https://doi.org/10.11604/pamj.2015.22.325.6990
|
| [24] |
Ozuah NW, Lubega J, Allen CE, et al. Five decades of low intensity and low survival: adapting intensified regimens to cure pediatric Burkitt lymphoma in Africa. Blood Adv 2020; 4: 4007–4019.
|
| [25] |
Wong ES, Choy RW, Zhang Y, et al. Global retinoblastoma survival and globe preservation: a systematic review and meta-analysis of associations with socioeconomic and health-care factors. Lancet Glob Health 2022; 10: e380–e389.
|
| [26] |
Liu B, Youlden DR, Wabinga H, et al. Survival from childhood cancer in Kampala, Uganda. Pediatr Blood Cancer 2021; 68: e28876.
|
| [27] |
Mostert S, Arora RS, Arreola M, et al. Abandonment of treatment for childhood cancer: position statement of a SIOP PODC Working Group. Lancet Oncol 2011; 12: 719–720.
|
| [28] |
Mansell R, Purssell E. Treatment abandonment in children with cancer in Sub-Saharan Africa: Systematic literature review and meta-analysis. J Adv Nurs 2018; 74: 800–808.
|
| [29] |
Williams LA, Spector LG. Survival Differences Between Males and Females Diagnosed With Childhood Cancer. JNCI Cancer Spectr 2019; 3: pkz032.
|
| [30] |
Molyneux EM, Rochford R, Griffin B, et al. Burkitt’s lymphoma. The Lancet 2012; 379: 1234–1244.
|
Cite This Article
-
APA Style
Lucien, D. D., Angèle, K., Rolande, K., Caroline, Y., Chantal, B., et al. (2025). High Mortality Rate Among Children and Adolescents with Cancer Treated in Burkina Faso. Central African Journal of Public Health, 11(6), 343-351. https://doi.org/10.11648/j.cajph.20251106.12
 Copy
|
Copy
|
 Download
Download
ACS Style
Lucien, D. D.; Angèle, K.; Rolande, K.; Caroline, Y.; Chantal, B., et al. High Mortality Rate Among Children and Adolescents with Cancer Treated in Burkina Faso. Cent. Afr. J. Public Health 2025, 11(6), 343-351. doi: 10.11648/j.cajph.20251106.12
Copy
|
Download
AMA Style
Lucien DD, Angèle K, Rolande K, Caroline Y, Chantal B, et al. High Mortality Rate Among Children and Adolescents with Cancer Treated in Burkina Faso. Cent Afr J Public Health. 2025;11(6):343-351. doi: 10.11648/j.cajph.20251106.12
Copy
|
Download
-
@article{10.11648/j.cajph.20251106.12,
author = {Dahourou Désiré Lucien and Kalmogho Angèle and Kabore Rolande and Yonaba Caroline and Bouda Chantal and Bouda Charlotte and Zoungrana Chantal and Ouédraogo Flore and Kouéta Fla},
title = {High Mortality Rate Among Children and Adolescents with Cancer Treated in Burkina Faso
},
journal = {Central African Journal of Public Health},
volume = {11},
number = {6},
pages = {343-351},
doi = {10.11648/j.cajph.20251106.12},
url = {https://doi.org/10.11648/j.cajph.20251106.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.cajph.20251106.12},
abstract = {Data on childhood cancer mortality are scarce in Burkina Faso. We estimated pediatric cancer mortality and identified its associated factors at the Yalgado Ouédraogo University Hospital Center (CHUYO) in Ouagadougou (Burkina Faso). We conducted a retrospective cohort study of children under the age of 15 admitted for cancer and treated at CHUYO between March 1, 2014, and December 31, 2017. The cumulative incidence of mortality and its associated factors were estimated with the risk of abandonment of treatment or follow-up as a competing risk. A total of 168 children/adolescents were included at a median age of 7 years (interquartile range [IQR]: 4–10 years); 71% were boys. The median follow-up duration was 4.51 person-months (IQR: 1.85-10.5). Burkitt lymphoma (77%) and retinoblastoma (21%) were the most common cancer. The majority of Burkitt lymphoma (90%) were diagnosed at stage 3/4; the abdominal (58%) and maxillofacial (23%) locations were the most common. All children/adolescents received chemotherapy and 10% received chemotherapy and surgery. No patients received radiotherapy. During follow-up, overall mortality was 46%, and the risk of abandonment was 39%. The cumulative incidence of mortality was 30, 43, and 45 per 100 person-months at 6, 12, and 24 months, respectively. In multivariate analysis, male gender (adjusted sub hazard ratio [aSHR]: 2.20; 95%CI: 1.13-4.27), abdominal localization (aSHR: 2.68; 95%CI: 1.24-5.78), maxillofacial and abdominal localization (aSHR: 3.39; 95%CI: 1.42-8.09) increased significantly the risk of death among children and adolescent treated for Burkitt lymphoma. Early diagnosis and improved access to treatment are essential for better survival rates among children and adolescents with cancer in Burkina Faso.
},
year = {2025}
}
Copy
|
Download
-
TY - JOUR
T1 - High Mortality Rate Among Children and Adolescents with Cancer Treated in Burkina Faso
AU - Dahourou Désiré Lucien
AU - Kalmogho Angèle
AU - Kabore Rolande
AU - Yonaba Caroline
AU - Bouda Chantal
AU - Bouda Charlotte
AU - Zoungrana Chantal
AU - Ouédraogo Flore
AU - Kouéta Fla
Y1 - 2025/11/03
PY - 2025
N1 - https://doi.org/10.11648/j.cajph.20251106.12
DO - 10.11648/j.cajph.20251106.12
T2 - Central African Journal of Public Health
JF - Central African Journal of Public Health
JO - Central African Journal of Public Health
SP - 343
EP - 351
PB - Science Publishing Group
SN - 2575-5781
UR - https://doi.org/10.11648/j.cajph.20251106.12
AB - Data on childhood cancer mortality are scarce in Burkina Faso. We estimated pediatric cancer mortality and identified its associated factors at the Yalgado Ouédraogo University Hospital Center (CHUYO) in Ouagadougou (Burkina Faso). We conducted a retrospective cohort study of children under the age of 15 admitted for cancer and treated at CHUYO between March 1, 2014, and December 31, 2017. The cumulative incidence of mortality and its associated factors were estimated with the risk of abandonment of treatment or follow-up as a competing risk. A total of 168 children/adolescents were included at a median age of 7 years (interquartile range [IQR]: 4–10 years); 71% were boys. The median follow-up duration was 4.51 person-months (IQR: 1.85-10.5). Burkitt lymphoma (77%) and retinoblastoma (21%) were the most common cancer. The majority of Burkitt lymphoma (90%) were diagnosed at stage 3/4; the abdominal (58%) and maxillofacial (23%) locations were the most common. All children/adolescents received chemotherapy and 10% received chemotherapy and surgery. No patients received radiotherapy. During follow-up, overall mortality was 46%, and the risk of abandonment was 39%. The cumulative incidence of mortality was 30, 43, and 45 per 100 person-months at 6, 12, and 24 months, respectively. In multivariate analysis, male gender (adjusted sub hazard ratio [aSHR]: 2.20; 95%CI: 1.13-4.27), abdominal localization (aSHR: 2.68; 95%CI: 1.24-5.78), maxillofacial and abdominal localization (aSHR: 3.39; 95%CI: 1.42-8.09) increased significantly the risk of death among children and adolescent treated for Burkitt lymphoma. Early diagnosis and improved access to treatment are essential for better survival rates among children and adolescents with cancer in Burkina Faso.
VL - 11
IS - 6
ER -
Copy
|
Download