Previous study was designed in two steps: flours formulation, improvement to traditional manufacturing processes and fortify five infant flours produced locally in Chad in vitamin A and zinc, iron and vitamin C. This study aimed to assess biological effectiveness of four improved and enriched experimental flours produced with local products on the iron status and speed of recovery in weight, height and MUAC of MAM children aged 6 to 59 months admitted at the Supplementary Nutrition Unit (UNS) of Notre Dame of Apostles Hospital (HNDA) at N'Djamena. The results of this study, which included 416 children, showed that moderately malnourished children under experimental flours enriched with dried Moringa leaf powder took a maximum of three weeks to recover from malnutrition. The Pennisetum typhoides flour with Moringa gave the best results, with 96% of children recovering after a duration of recovery of 17.5 days. Children under red sorghum flour from Bongor without Moringa showed the highest daily weight gain in the study, at 8 g/kg-body weight per day. The same flour with Moringa showed the highest hemoglobin gain of 13.5 g/dl. Children under maize flour without Moringa took the longest to recover in the study, an average of 32.7 days. In conclusion, Pennisetum typhoides and red sorghum flours with Moringa can make a valid contribution to reducing the prevalence of malnutrition in children.
| Published in | Central African Journal of Public Health (Volume 10, Issue 6) |
| DOI | 10.11648/j.cajph.20241006.17 |
| Page(s) | 285-296 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2024. Published by Science Publishing Group |
Chad Infant Formula, Nutritional Assessment, Moringa oleifera, Iron, Biological Effectiveness
Flours | Girls | Boy | Total |
|---|---|---|---|
MNM | 24 | 28 | 52 |
MNSM | 15 | 37 | 52 |
PNM | 20 | 32 | 52 |
PNSM | 13 | 39 | 52 |
SRBM | 25 | 27 | 52 |
SRBSM | 20 | 32 | 52 |
SRKM | 28 | 24 | 52 |
SRKSM | 25 | 27 | 52 |
Total | 170 | 246 | 416 |
[6 - 12[ | [12 - 18[ | [18 - 24[ | [24 - 30[ | [30 - 36[ | [36 - 42[ | [42 - 48[ | [48 - 54[ | Total | |
|---|---|---|---|---|---|---|---|---|---|
MNM | 21 | 17 | 8 | 6 | 0 | 0 | 0 | 0 | 52 |
MNSM | 15 | 26 | 5 | 3 | 3 | 0 | 0 | 0 | 52 |
PNM | 28 | 8 | 11 | 4 | 0 | 0 | 0 | 1 | 52 |
PNSM | 18 | 21 | 6 | 6 | 1 | 0 | 0 | 0 | 52 |
SRBM | 25 | 18 | 6 | 2 | 1 | 0 | 0 | 0 | 52 |
SRBSM | 16 | 17 | 12 | 6 | 1 | 0 | 0 | 0 | 52 |
SRKM | 23 | 15 | 9 | 4 | 0 | 1 | 0 | 0 | 52 |
SRKSM | 19 | 23 | 2 | 5 | 1 | 2 | 0 | 0 | 52 |
Total | 165 | 145 | 59 | 36 | 7 | 3 | 0 | 1 | 416 |
Flours | PNM | MNM | PNSM | SRBM | SRKM | SRKSM | SRBSM | MNSM |
|---|---|---|---|---|---|---|---|---|
Average duration of recovery (days) | 17,5 | 18,6 | 20,1 | 21, 2 | 22,3 | 24,6 | 27,3 | 32,7 |
Flours | PNM | MNM | PNSM | SRBM | SRKM | SRKSM | SRBSM | MNSM |
|---|---|---|---|---|---|---|---|---|
Average weight gain g/kg/day | 6,75 | 6,29 | 6,63 | 5,50 | 5,93 | 4,87 | 8,00 | 5,81 |
BMI | Body Mass Index |
IPC | Integrate Food Security Phase Classification |
MAM | Moderately Acutely Malnourished |
MAS | Severely Acutely Malnourished |
MUAC | Mid-upper Arm Circumference |
HNDA | Notre Dame of Apostles Hospital |
SMART | Standardized Monitoring and Assessment of Relief and Transitions |
UNS | Supplementary Nutritional Unit |
UNT | Therapeuutic Nutritionnal Unit |
NCHS | National Center for Health Statistics of United States of America |
ABUM | Burkinabe Association of Misola |
UNICEF | United Nations Children's Fund |
P/T | Weight-for-height Index |
P/A | Weight-for-age Index |
T/A | Height for Age Index |
ANOVA | Analysis of Variance |
SPSS | Statistical Package for Social Sciences |
CREN MORIJA | Recovery and Nutritional Education Center of MORIJA at Ouagadougou |
CRSBAN | Centre for Research in Biological, Food and Nutritional Sciences |
| [1] | IPC. Analyse IPC de la malnutrition aiguë, Octobre 2020 – septembre 2021. Publié en Avril 2021. |
| [2] | Ministère de la Santé Publique du Tchad. Enquête nationale de nutrition et de mortalité rétrospective. Rapport final. Décembre 2022. |
| [3] | Compaoré WR, Nikièma PA, Savadogo A, Bassole HIN, Mouecoucou J, Pignatelli S, Simporé J, Traoré SA. Nutritional and Hematological Recovery of Severely Malnourished Children with New Flour Formulas Developed at Ouagadougou (Burkina Faso). British Journal of Dairy Sciences. 2011; 2(1): 11–17. |
| [4] | Yomadji-Outangar O. Fabrication de farines enrichies à partir de produits locaux du Tchad. Centre National de Nutrition et de Technologie Alimentaire. N’Djaména, Tchad; 1995. |
| [5] | Hamza OB, Guiral C, Esaie DD, Ndingambaye K, Diallo P, Batakao G, Naibé N, Syntiche ND and Noumassei H. Rapport descriptif de l'Enquête Nationale sur l'Etat Nutritionnel et l'Alimentation au Tchad. Ministère de la Santé Publique. République du Tchad, 2002. |
| [6] | Traore T. Élaboration et évaluation d’une stratégie d’amélioration de l’alimentation de complément des jeunes enfants au Burkina Faso. Doctoral Thesis. Université de Ouagadougou, UFR-SVT, CRSBAN; 2005. 233 pages. |
| [7] | Zongo U. Etude de l’évolution des paramètres cliniques et biologiques des enfants vulnérables dont le régime alimentaire inclut la poudre de feuilles de Moringa. DEA Research Dissertation. Université de Ouagadougou, Burkina Faso; 2012. 59 pages. |
| [8] | Gning RD, Ndong M, Wade S, Dossou N et Guiro AT. (2007). Valeur nutritionnelle du Moringa oleifera, étude de la biodisponibilite du fer, effet de l'enrichissement de divers plats traditionnels sénégalais avec la poudre des feuilles. African Journal of Food, Agriculture, Nutrition and Development. 17 pages. |
| [9] | Tété-Bénissan A, Lawson-Evi KA, Kokou K and Gbéassor M. Effet de la poudre des feuilles Moringa oleifera Lam. sur l’évolution du profil de l’hémogramme des enfants malnutris au Togo: Evaluation chez les sujets HIV positifs. African Journal of Food, Agriculture, Nutrition and Développent 2012: 12(2): 6007-6026. |
| [10] | Shakir A. and Morley D. Measuring malnutrition. The Lancet, volume 303, Issue 7860, pages 758-759, April 20, 1974. |
| [11] | WHO (2001). Iron Deficiency Anemia: Assessment, Prevention, and Control. A guide for program managers. WHO/NHD/013. |
| [12] | Savadogo B. Statut nutritionnel et parasitoses chez les enfants au Burkina Faso: cas des Provinces du Kadiogo, d’Oubritenga et du Sourou. Doctoral Thesis. Université Ouaga I Professeur Joseph KI-ZERBO, UFR-SVT, ED/ST; 2016. 156 pages. |
| [13] | Dossou, IN, S Wade, AT Guiro, CS, Sarr, B. Diaham, D. Cissé, JP Beau, P Chappuis, D Hoffman and D. Lemonnier. Nutritional status of preschool Senegalese children: long-term effects of early severe malnutrition. Br. J. Nutr., 90: 1123-1132. |
| [14] | Diouf S, Folquet M, Mbofung K, Ndiaye O, Brou K, Dupont C, N’dri D, Vuillerod M, Azais-Braesco V, Tetanye E. (2015). Prévalence et déterminants de l’anémie chez le jeune enfant en Afrique francophone-Implication de la carence en fer. Elsevier Masson SAS. Archives de pédiatrie 2003; 22: 1188-1197. |
| [15] | Nassaradine MM, Yacoub MA, Emmanuel I, Mahamat B, Amadou SD, Abelsalam T and Magassouba D. Impact of therapeutic foods on the staturo-weight and hematological parameters of Malnourished children at the therapeutic nutritional unit of Mongo (chad). International Journal of Science Academic Research, Vol. 02, Issue 09, pp.3041-3042, September, 2021. |
| [16] | Thierno M. MILLIMONO, Fanta TOURE, Ahmadou S. DIALLO, Ibrahim F. BAMBA. Assessment of children care aged 6 to 59 months suffering from moderate acute malnutrition in the Learning and Nutritional Rehabilitation Homes in Kouroussa prefecture. Nutr. Santé, 2019, Vol. 08, N°02: 42-50. |
| [17] | Amadou MAR, Mahamadou L, Yaou C, Alpha GB, Alkassoum I, Houa SS, Hassoumi S. Qualité nutritionnelle et sensorielle d’une farine infantile enrichie au soja et à la spiruline et test de récupération nutritionnelle chez les enfants de 6 à 24 mois au Niger. International Journal of Advances in Engineering and Management (IJAEM) Volume 3, Issue 7 July 2021, pp: 633-647. |
| [18] | Bidossessi VS HOUNDJI, Sam F. BODJRENOU, Serge BM LONDJI, Romaric OUETCHEHOU, Alfred ACAKPO, Kou’Santa Sabiba E. AMOUZOU et HOUNMENOU. Amélioration de l’état nutritionnel des enfants âgés de 6 à 30 mois à Lissèzoun (Centre-Bénin) par la poudre de feuilles de Moringa oleifera (Lam.). Int. J. Biol. Chem. Sci. 7(1): 225-235, 2013 |
| [19] | Ashworth A. and Millard DJ. (1986). Catch-up growth in children. Nutrition Reviews 44: 157-163. |
| [20] | Manary MJ, Ndekha PA, Maleka K and Briend A. Home based therapy for severe malnutrition with ready-to-use food. Archives of Disease in Childhood 2004). 89: 557-561. |
| [21] | Adam, OY, Soudy, ID, Ousman, AH, Kanika, MA and Garba M. (2023). Effectiveness of Enriched Flour in the Recovery of Children Aged 6 to 59 Months with Moderate Acute Malnutrition. Food and Nutrition Sciences, 14, 687-697. |
| [22] | Cook JD. (1990). Adaptation in iron metabolism. American Journal of Clinical Nutrition 51, 301-308. |
| [23] | Raouda MY. Effet des feuilles de Moringa oleifera sur les paramètres anthropométriques, hématologiques et biologiques des enfants bien portants en âge scolaire à Yagoua (Nord Cameroun). Doctoral Thesis. Université de N’Djaména, FSSH; 2013. 101 pages. |
APA Style
Kayalto, B., Kimassoum, D., Otchom, B. B., Soubeiga, E., Traore, A. S. (2024). Assessment of Biological Effectiveness of Infant Flours on the Iron Status and Speed of Recovery of MAM Children Admitted to HNDA Hospital at N'Djamena (Chad). Central African Journal of Public Health, 10(6), 285-296. https://doi.org/10.11648/j.cajph.20241006.17
ACS Style
Kayalto, B.; Kimassoum, D.; Otchom, B. B.; Soubeiga, E.; Traore, A. S. Assessment of Biological Effectiveness of Infant Flours on the Iron Status and Speed of Recovery of MAM Children Admitted to HNDA Hospital at N'Djamena (Chad). Cent. Afr. J. Public Health 2024, 10(6), 285-296. doi: 10.11648/j.cajph.20241006.17
AMA Style
Kayalto B, Kimassoum D, Otchom BB, Soubeiga E, Traore AS. Assessment of Biological Effectiveness of Infant Flours on the Iron Status and Speed of Recovery of MAM Children Admitted to HNDA Hospital at N'Djamena (Chad). Cent Afr J Public Health. 2024;10(6):285-296. doi: 10.11648/j.cajph.20241006.17
@article{10.11648/j.cajph.20241006.17,
author = {Barnabas Kayalto and Djimadoum Kimassoum and Brahim Boy Otchom and Emilienne Soubeiga and Alfred Sadjo Traore},
title = {Assessment of Biological Effectiveness of Infant Flours on the Iron Status and Speed of Recovery of MAM Children Admitted to HNDA Hospital at N'Djamena (Chad)
},
journal = {Central African Journal of Public Health},
volume = {10},
number = {6},
pages = {285-296},
doi = {10.11648/j.cajph.20241006.17},
url = {https://doi.org/10.11648/j.cajph.20241006.17},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.cajph.20241006.17},
abstract = {Previous study was designed in two steps: flours formulation, improvement to traditional manufacturing processes and fortify five infant flours produced locally in Chad in vitamin A and zinc, iron and vitamin C. This study aimed to assess biological effectiveness of four improved and enriched experimental flours produced with local products on the iron status and speed of recovery in weight, height and MUAC of MAM children aged 6 to 59 months admitted at the Supplementary Nutrition Unit (UNS) of Notre Dame of Apostles Hospital (HNDA) at N'Djamena. The results of this study, which included 416 children, showed that moderately malnourished children under experimental flours enriched with dried Moringa leaf powder took a maximum of three weeks to recover from malnutrition. The Pennisetum typhoides flour with Moringa gave the best results, with 96% of children recovering after a duration of recovery of 17.5 days. Children under red sorghum flour from Bongor without Moringa showed the highest daily weight gain in the study, at 8 g/kg-body weight per day. The same flour with Moringa showed the highest hemoglobin gain of 13.5 g/dl. Children under maize flour without Moringa took the longest to recover in the study, an average of 32.7 days. In conclusion, Pennisetum typhoides and red sorghum flours with Moringa can make a valid contribution to reducing the prevalence of malnutrition in children.
},
year = {2024}
}
TY - JOUR T1 - Assessment of Biological Effectiveness of Infant Flours on the Iron Status and Speed of Recovery of MAM Children Admitted to HNDA Hospital at N'Djamena (Chad) AU - Barnabas Kayalto AU - Djimadoum Kimassoum AU - Brahim Boy Otchom AU - Emilienne Soubeiga AU - Alfred Sadjo Traore Y1 - 2024/12/27 PY - 2024 N1 - https://doi.org/10.11648/j.cajph.20241006.17 DO - 10.11648/j.cajph.20241006.17 T2 - Central African Journal of Public Health JF - Central African Journal of Public Health JO - Central African Journal of Public Health SP - 285 EP - 296 PB - Science Publishing Group SN - 2575-5781 UR - https://doi.org/10.11648/j.cajph.20241006.17 AB - Previous study was designed in two steps: flours formulation, improvement to traditional manufacturing processes and fortify five infant flours produced locally in Chad in vitamin A and zinc, iron and vitamin C. This study aimed to assess biological effectiveness of four improved and enriched experimental flours produced with local products on the iron status and speed of recovery in weight, height and MUAC of MAM children aged 6 to 59 months admitted at the Supplementary Nutrition Unit (UNS) of Notre Dame of Apostles Hospital (HNDA) at N'Djamena. The results of this study, which included 416 children, showed that moderately malnourished children under experimental flours enriched with dried Moringa leaf powder took a maximum of three weeks to recover from malnutrition. The Pennisetum typhoides flour with Moringa gave the best results, with 96% of children recovering after a duration of recovery of 17.5 days. Children under red sorghum flour from Bongor without Moringa showed the highest daily weight gain in the study, at 8 g/kg-body weight per day. The same flour with Moringa showed the highest hemoglobin gain of 13.5 g/dl. Children under maize flour without Moringa took the longest to recover in the study, an average of 32.7 days. In conclusion, Pennisetum typhoides and red sorghum flours with Moringa can make a valid contribution to reducing the prevalence of malnutrition in children. VL - 10 IS - 6 ER -
Department of Life and Earth Sciences, Bongor Teachers' Training Higher School, Bongor, Chad
Research Fields: Human nutrition, Infant flours, food microbiology, food quality, Water pollution by heavy metals, Pesticide residues in food
Faculty of Human Health Sciences, University of N’Djamena, N'Djamena, Chad
Research Fields: Food safety, Nutrition, Food microbiology, Food quality, Dietetics, Food technology
Department of Biology, Faculty of Exact and Applied Sciences, University of N’Djamena, N'Djamena, Chad
Research Fields: Biochemistry
Department of Biochemistry and Microbiology, Centre for Research in Biological, Food and Nutritional Sciences, Training and Research Unit of Life and Earth Sciences, University of Ouagadougou I Pr Joseph KI ZERBO, Ouagadougou, Burkina Faso
Research Fields: Human nutrition, applied microbiology, Microbial biotechnology, PCR, Biochemistry
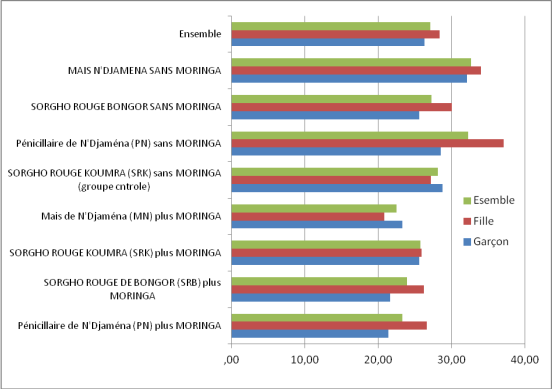
Figure 1. Duration of recovery of children, in days, at the UNS by flour and gender.

Figure 2. Weight evolution of children at inclusion and discharge.

Figure 3. Evolution of weight (kg) during treatment.
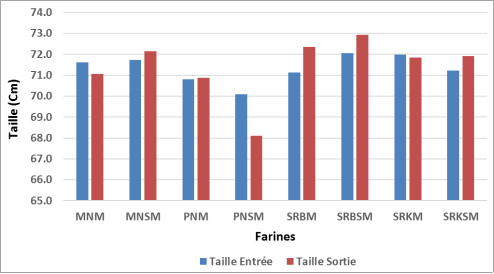
Figure 4. Evolution of children’s height from inclusion to discharge.

Figure 5. Evolution of height gain during study.
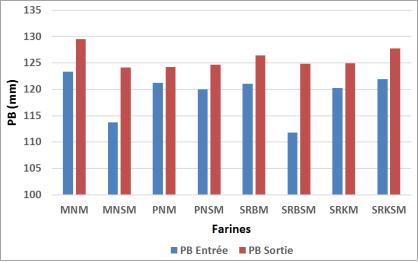
Figure 6. Evolution of MUAC at inclusion and discharge.
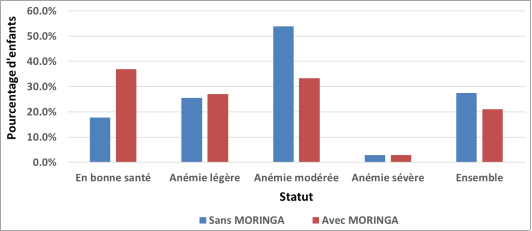
Figure 7. Hemoglobin status of children at discharge.
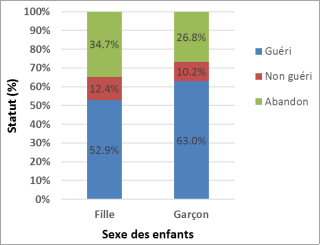
Figure 8. Cure and drop-out rates by sex of child.

